
Respiratory Syncytial Virus (RSV) remains a persistent, year-round threat to infants and young children, often leading to severe respiratory tract infections and hospitalizations. While awareness remains low, medical experts emphasize that healthy, full-term babies are frequently affected, with the virus carrying long-term risks for conditions like asthma and recurrent wheezing.
The Hidden Burden of RSV in Infants
While many parents associate winter months with respiratory illnesses, RSV is a perennial virus that typically peaks between September and December. The virus is highly contagious; statistics indicate that two out of three children experience their first infection before their first birthday. For the most vulnerable—infants aged six months and below—RSV accounts for 81.3% of viral respiratory tract infections.
Although infants with underlying conditions like cardiac malformations or neurological disorders are at higher risk, the impact extends far beyond those groups. More than 80% of severe RSV cases involve children who were born at full term with no underlying health issues. Symptoms often mimic common colds, starting with cough, runny nose, and fever, but can rapidly escalate into severe respiratory distress, including bronchospasms, chest indrawing, and the need for mechanical ventilation.
Hospitalization Costs and Long-Term Health Risks
The clinical impact of RSV is matched by a significant strain on healthcare resources. Because 84.5% of infected children under two years old require hospitalization, the economic burden is substantial. A median hospital stay for an RSV patient costs approximately USD756, a figure that does not account for the indirect costs of parental income loss during the recovery period.
Beyond the immediate hospital visit, the virus carries long-term consequences for a child’s development. Research cited by pediatricians suggests that an RSV infection can increase the risk of developing asthma by up to 12 times. Children may also suffer from abnormal lung function and recurrent wheezing long after the initial infection has cleared, complicating their health profile for years.
Monitoring Respiratory Trends Beyond RSV
While RSV represents a consistent danger to pediatric populations, public health agencies like the Centers for Disease Control and Prevention (CDC) track a variety of other respiratory germs that cause overlapping symptoms. Currently, parainfluenza virus (PIV) activity is elevated nationally, while rhinovirus/enterovirus (RV/EV) levels are trending downward.

The CDC notes that these viruses, like RSV, can cause fever, congestion, and shortness of breath, sometimes progressing to pneumonia. Unlike some other illnesses, there are currently no vaccines available for PIV or RV/EV, making hygiene practices such as hand washing and surface cleaning the primary defense. Additionally, while pertussis—commonly known as whooping cough—is circulating, the CDC reports that cases have remained lower than the peak seen in November 2024.
Preventive Strategies and Parental Vigilance
Because there is no lasting immunity to RSV—meaning a child can be infected multiple times—prevention is the primary strategy for managing the virus. Pediatricians recommend breastfeeding as a foundational step, as human milk provides immune and antiviral components that may help protect infants. Parents are encouraged to remain vigilant for signs of distress, such as lethargy, poor feeding, or rapid, shallow breathing, which signal a need for urgent medical care.
For parents concerned about respiratory symptoms, the best course of action remains consulting a healthcare provider to distinguish RSV from other circulating illnesses. As the medical community continues to monitor these trends, the focus remains on early recognition of severe symptoms to prevent the need for intensive care interventions.
Worth a look
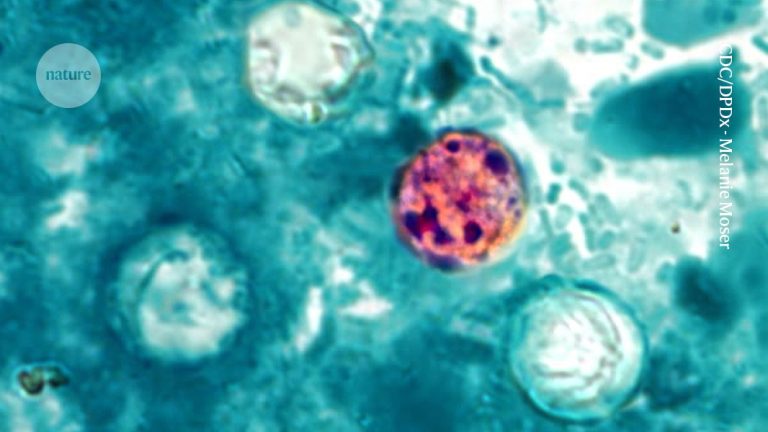
Cyclospora Parasite Outbreak Surges Across United States as Cases Climb
Health officials are investigating a surging outbreak of Cyclospora cayetanensis, a parasite causing prolonged intestinal distress across the...

Kyrgyzstan Conducts Emergency Drills Ahead of 2026 World Nomad Games
Kyrgyzstan has conducted large-scale, interagency public health emergency exercises in Cholpon-Ata as part of its preparations for the...

Black Women Face Higher Breast Cancer Mortality
Black women in Canada and the United States face significantly higher breast cancer mortality rates and later-stage diagnoses...

Thailand Probes Six Hospitals Over Fraudulent Citizenship Birth Scheme
BANGKOK — Thai health authorities are investigating six private hospitals over suspected fraudulent birth registrations that may have...